1 Human Engineering Research Laboratories, Department of Veterans Affairs, Pittsburgh, PA
2 Department of Bioengineering, University of Pittsburgh, Pittsburgh, PA
3 Department of Physical Medicine and Rehabilitation, University of Pittsburgh, Pittsburgh, PA
4 Deptartment of Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA
5 Landstuhl Regional Medical Center, Landstuhl, Germany
Abstract
There are limited data on the prevalence of upper extremity nerve entrapments in military veterans with major limb amputations. A pilot study of 20 participants at the 2008 National Disabled Veterans Winter Sports Clinic (NDVWSC) used nerve conduction studies and showed an increased prevalence of upper extremity nerve entrapments in the veteran amputee population. In this study, we followed on the previous findings of increased prevalence of upper extremity nerve entrapments. Using ultrasonography techniques, we investigated changes in the median nerve characteristics in a sample of 36 veterans. The results were in agreement with those of the previous pilot study and demonstrated evidence of median nerve health deterioration in the veterans with major limb amputations.
Keywords:
nerve entrapment; median nerve; major limb amputations; carpal tunnel syndrome; ultrasonography
Background
Individuals with lower extremity amputations rely heavily on their upper extremities for activities of daily living and mobility. Both manual wheelchair propulsion and crutch ambulation have been implicated in upper limb repetitive strain injuries, including upper extremity nerve entrapment conditions, such as carpal tunnel syndrome (CTS). The prevalence of CTS among manual wheelchair users is between 49% and 73%. Gellman, in a study of 77 individuals with T2 or below paraplegia, found 49% had signs and symptoms of CTS (1). Sie interviewed 103 subjects with paraplegia and found historical or physical examination evidence of CTS in 66% (2). In these studies, wheelchair propulsion and crutch use have been implicated as contributing to injury. There is, however, limited data on the incidence of upper extremity nerve entrapments in the population of individuals with major limb loss, especially among soldiers and veterans. Reddy reported on carpal and cubital syndromes in 5 patients with a contralateral upper extremity amputation that resolved with adjustment of the figure-8 harness (3). Boninger, Robertson, Wolff, and Cooper (4) showed that although elite wheelchair users had a higher prevalence of carpal tunnel syndrome than the general population, these wheelchair athletes had a similar or lower prevalence than reported in the general wheelchair using population. In manual wheelchair users, several variables have been shown to correlate with median nerve function. These include body mass and wheelchair pushrim forces (5), and wrist forces and moments (6, 7). Crutch ambulators are likely subject to similar forces, but this has yet to be quantified. Individuals with disabilities have reported that acquiring a repetitive strain injury is similar to having a more severe disability, and that the accompanying pain is one of the most significant factors related to self-reported quality of life. The objective of this research study was to use ultrasonography to investigate nerve entrapments of the upper extremities in soldiers/veterans with major limb loss. This information is needed to guide the development and evaluation of prevention and treatment approaches.
Methodology
Subjects
Thirty-six veterans or active duty soldiers with at least one major limb amputation were recruited from participants at the 2009 National Disabled Veterans Winter Sports Clinics at Snowmass, Colorado. All subjects were aged 18 and over and used assistive technology, such as a wheelchair or prosthesis, for mobility or to assist with activities of daily living. Subjects completed a questionnaire, and underwent an upper extremity physical exam and quantitative clinical ultrasonographic evaluation.
Ultrasonography (US)
Ultrasonographic images were collected using the Philips HD11 1.0.6 ultrasound machine with a 5-12 MHz 50 mm linear array transducer. Images of the carpal tunnel, with primary emphasis on the median nerve, were collected at the distal radius and the pisiform level. These two regions are easily viewed using US and nerve characteristics at these locations have previously been linked to CTS both symptomatically and electrodiagnostically (8-12).
Data Analysis
An interactive MATLAB image analysis program was used to make manual diameter and cross-sectional area (CSA) measurements of structures of interest using the US images. This program has been used in previous studies (13-15). Median nerve diameter and cross-sectional area were determined by performing a boundary trace (Figure 1). Other indicators such as flattening ratio and swelling ratio were determined post-analysis.
Statistical Analysis
Distributions of variables were examined and transformations were made where necessary. Paired t-tests were conducted to determine significant differences between the variables at two levels, and p-values of 0.05 were considered significant.
Results
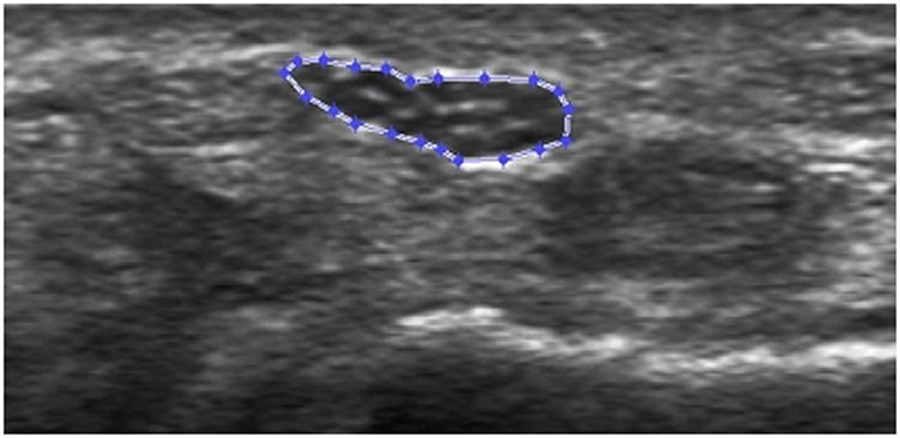 Figure 1: An exemplar US image of median nerve at the distal radius level that has been analyzed using our image analysis software.
Figure 1: An exemplar US image of median nerve at the distal radius level that has been analyzed using our image analysis software.The changes in ultrasonographic parameters were not statistically significant; however, trends which may represent deteriorating median nerve health were noted in our analysis. Particularly, the flattening ratio (defined as nerve width divided by nerve height) at the pisiform level was greater when compared to those at the distal radius level. While the average cross-sectional area at the pisiform level was not significantly different from the CSA at the distal radius level, the swelling ratio (defined as CSA at the pisiform level / CSA at the distal radius level) showed 4.2% increase (Table 1).
|
Cross-sectional Area |
Flattening Ratio |
Swelling Ratio |
|---|---|---|---|
Distal Radius Level |
9.45 ± 1.54 |
3.27 ± 0.80 |
100.5% ± 30.2% |
Pisiform Level |
9.33 ± 2.63 |
3.41 ± 1.25 |
Discussion
There are limited data on the prevalence of upper extremity nerve entrapments in military veterans with major limb loss. Because many service members with amputations are returning to service and veterans with major limb amputations provide a model for the future of recent international conflicts (e.g., Operation of Iraqi Freedom and Operation of Endurance Freedom) veterans, information on the incidence of upper extremity nerve entrapments is important for counseling and safety training for military personnel and veterans, for training medical staff, and for preparing strategies for prophylaxis and treatment. A pilot study of 20 participants was performed using nerve conduction studies at the 2008 National Disabled Veterans Winter Sports Clinic and showed an increased prevalence of upper extremity nerve entrapments in the veteran amputee population. The objective of the current study was to use ultrasound to follow on those findings of increased prevalence of upper extremity nerve entrapments with a larger subject population.
Ultrasonography has been proved to be a reliable and repeatable means to investigate musculoskeletal structures. Research has shown good reproducibility of median nerve characteristics when measured using ultrasound (16). An unpublished repeatability study conducted by the same investigators collecting and analyzing these images in 20 subjects, found up to 91% intra-class correlation coefficients. Ultrasound provides investigators with a non-invasive, relatively inexpensive, and dynamic method to evaluate musculoskeletal structures, such as tendon and peripheral nerves, even in a non-clinical environment. Our laboratories have successfully used ultrasound to study structural changes in upper extremity, including tendons and nerves in shoulder and wrist areas.
The results of current study demonstrated that even though ultrasound characteristics of the amputees’ median nerve were not statistically different, trends representing deterioration of median nerve health were noted. This study correlated with the findings of our pilot study where all 20 participants had electrodiagnostic evidence of nerve entrapment. Multiple variables may contribute to these injuries and more research is necessary to investigate possible causes and prevention. By gaining more information regarding the median nerve health in major limb amputees we can reduce the risk of injury and perhaps delay the onset of nerve damage. Longitudinal studies have yet to be conducted and vigorous statistical analysis in a much larger population must be performed, as this small study might have not possessed enough power to detect a significant difference.
REFERENCES
- Gellman, H., Chandler, D. R., Petrasek, J., Sie, I. H., Adkins, R. H., & Waters, R. L. (1998). Carpal tunnel syndrome in paraplegic patients. J Bone Joint Surg [Am], 70, 517-519.
- Sie, I. H., Waters, R. L., Adkins, R. H., & Gellman, H. (1992). Upper extremity pain in the postrehabilitation spinal cord injured patient. Arch Phys Med Rehabil, 73, 44-48.
- Reddy, M. P. (1984). Nerve entrapment syndromes in the upper extremity contralateral to amputation. Arch Phys Med Rehabil. 65(1), 24-6.
- Boninger, M. L., Robertson, R. N., Wolff, M., & Cooper, R. A. (1996). Upper limb nerve entrapments in elite wheelchair racers. Am J Phys Med and Rehab, 75(3), 170-6.
- Baldwin, M. A, Boninger, M. L, Shimada, S. D., Cooper, R. A, & O’Conner, T. J. (1998). A relationship between pushrim kinetics and median nerve dysfunction. Proc. RESNA Annual Conference, 378-380.
- Shimada, S. D., Boninger, M. L, Cooper, R. A., & Baldwin, M. A. (1998). A relationship between wrist biomechanics during wheelchair propulsion and median nerve dysfunction. Proc. RESNA Annual Conference, 128-130.
- Fay, B. T., Boninger, M. L., Cooper, R. A., Baldwin, M. A., & Koontz, A. M. (1999). Wrist kinematics and indications of carpal tunnel syndrome during manual wheelchair propulsion. Proc. 1st Joint BMES/EMBS Conf., 628.
- Buchberger, W., Judmaier, W., Birbamer, G., Lener, M., & Schmidauer, C. (1992). Carpal tunnel syndrome: diagnosis with high-resolution sonography. AJR Am J Roentgenol, 159(4), 793-8.
- Chen, P., Maklad, N., Redwine, M., & Zelitt, D. (1997). Dynamic high-resolution sonography of the carpal tunnel. AJR Am J Roentgenol, 168(2), 533-7.
- Duncan, I., Sullivan, P., Lomas, F. (1999). Sonography in the diagnosis of carpal tunnel syndrome. AJR Am J Roentgenol, 173(3), 681-4.
- Keberle, M., Jenett, M., Kenn, W., Reiners, K., Peter, M., Haerten, R,. Hahn. D. (2000). Technical advances in ultrasound and MR imaging of carpal tunnel syndrome. Eur Radiol, 10(7), 1043-50.
- Keles, I., Karagulle Kendi, A. T., Aydin, G., Zog, S. G., & Orkun, S. (2005). Diagnostic precision of ultrasonography in patients with carpal tunnel syndrome. Am J Phys Med Rehabil, 84(6), 443-50.
- Collinger, J. L., Gagnon, D., Jacobson, J., Impink, B. G., & Boninger, M. L. (2009). Reliability of quantitative ultrasound measures of the biceps and supraspinatus tendons. Acad Radiol, 16(11), 1424-32.
- Impink, B. G., Boninger, M. L., Walker, H., & Collinger, J. L. (2009) Ultrasonographic median nerve changes after a wheelchair sporting event. Arch Phys Med Rehabil, 90(9), 1489-94.
- Brose, S. W., Boninger, M. L., Fullerton, B., McCann, T., Collinger, J. L, Impink, B. G, & Dyson-Hudson, T. A. (2008). Shoulder ultrasound abnormalities, physical examination findings, and pain in manual wheelchair users with spinal cord injury. Arch Phys Med Rehabil, 89(11), 2086-93.
- Aleman, L., Berna, J. D., Reus, M., Martinez, F., Domenech-Ratto, G., & Campos, M. (2008) Reproducibility of sonographic measurements of the median nerve. J Ultrasound Med, 27(2), 193-7.
ACKNOWLEDGEMENTS
This material is the result of work supported with resources and the use of facilities at the Human Engineering Research Laboratories, VA Pittsburgh Healthcare System, and the following funding sources: Center for Excellence for Wheelchairs and Associated Rehabilitation Engineering (B3142C), the Paralyzed Veterans of America, and the NIH Training Rehabilitation Clinicians for Research Careers (T32 HD049307).
Author Contact Information:
Kevin K. Toosi
Human Engineering Research Laboratories
7180 Highland Drive
Building 4, 2nd Floor, East Wing, 151R-1
Pittsburgh, PA 15206
Phone: 412-954-5282
E-mail: kkt6@pitt.edu